NO SURGERY
Breast Tumor Ablation
Breast cancer surgery has evolved considerably since the days of those draconian radical mastectomies and disfigurement, to a far more conservative surgical approach today!
Yet, many requisite breast tumor resections – particularly within the EU -- have now been replaced with safe and effective thermal ablations (either cryoablation or microwave ablation) with considerable rarity in the U.S. because of the lack of FDA approval, and no health insurance reimbursement.
Microwave breast tumor ablation (MWA) is one of the newer modalities of thermal ablation which has been proven to be safe and effective in the destruction of many primary and metastatic breast tumors. MWA uses electromagnetic waves to produce a “directed” heat that destroys the cancerous tumor cells without requiring surgery or causing body disfigurement.
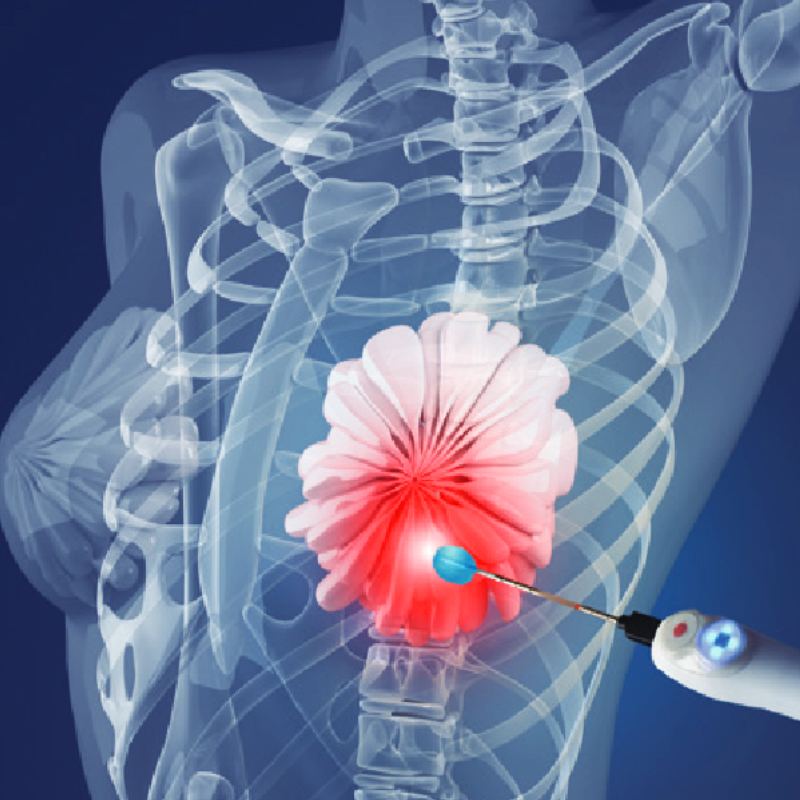
MWA is a minimally invasive technique widely used in the treatment of tumors of various organs. A microwave breast tumor ablation is similar to an ultrasound-guided needle biopsy performed by an interventional radiologist with the patient awake and comfortable.
Once the probe has entered the tumor cells, extreme heat is transmitted directly into the cancerous tumor cells, causing instantaneous cell death/destruction (well within preset margins) without causing harm to healthy tissue.
Pts can undergo MWA multiple times, either singularly or with other treatments if indicated.
The advantages of MWA as compared to conventional surgery, are faster recovery, reduced morbidity and mortality, minimal, if any, body disfigurement, accurate targeting under ultrasound or CT guidance, short outpatient treatment, and easily repeatable if residual lesions reappear.
MWA Preparation
The procedure begins with an ultrasound detecting the exact location of the cancer breast tumor, followed by a local anesthetic injected into the skin above the targeted area. A small (3mm) skin incision is made. Followed by a needle-like instrument called a probe inserted through the incision and placed into the center of the tumor. The procedure takes approximately 30 minutes, with the entire process taking about 1 hour from start to finish.
Post MWA Expectations
Notify ICCA if
Potential Imaging Deficiencies
There is a large body of evidence that MWA effectively destroys multiple cancer types. However, the key requirement for successful MWA is a well-defined tumor that can be accurately targeted.
Unfortunately, the complete extent of breast cancer might not be detectable on mammography, ultrasound, MRI, or thermography – which is why a PET/CT is often the preferred imaging of choice.
This is especially true for non-invasive breast cancer or ductal carcinoma in situ (DCIS), which is typically invisible unless it is associated with microcalcifications. DCIS co-exists with most invasive breast cancer, and may also extend a few millimeters or more beyond the main cancer mass.
There may also be small, undetectable areas of invasive cancer outside the main tumor. Unlike surgery, which permits microscopic examination of the surgical margins to determine if cancer extends beyond the visible tumor, MWA does not facilitate microscopic examination of the tissue surrounding the visible tumor. Consequently, when MWA is performed for breast cancer, our physicians intentionally ablate an area 1-2 cm beyond the visible tumor to treat undetectable DCIS and/or invasive cancer in the immediate perimeter of the visible tumor.
MWA and DCIS
Many patients with DCIS (ductal carcinoma in situ, non-invasive breast cancer, or stage 0 breast cancer) can undergo MWA. Requirements include a small area of involvement (typically 4.5 cm or less) and DCIS that is visible by ultrasound since MWA is usually performed under ultrasound guidance.
When DCIS is not visible by ultrasound, the treating physician can arrange for the insertion of an ultrasound-visible marker in the center of the area of DCIS (or next to your existing biopsy site marker), which is used as a target for the MWA procedure.
Placement of the ultrasound-visible marker is usually performed under stereotactic or mammographic guidance using a procedure similar to your original stereotactic needle biopsy. In some cases, the marker placed at the time of the original needle biopsy is already ultrasound visible. When this is the case, the placement of another ultrasound-visible marker is unnecessary. Our treating physicians will review your mammogram, ultrasound, and MRIs to assess your eligibility for MWA, and to determine if placement of an ultrasound-visible marker is needed.
MWA followed by Short-course Radiation and/or Chemotherapy
One of the major misconceptions about MWA is that it completely replaces the need for radiation or systemic medicines. Radiation is usually recommended with surgery to treat undetected residual disease in the surrounding breast, skin, or lymph nodes. The addition of radiation to surgery is generally associated with a 60% reduction in the risk of recurrence in the breast and lymph node area. Moreover, nearly all breast cancer patients with metastatic nodes should consider undergoing radiation pre- or post-micro ablation!
Drug therapies like anti-estrogen therapy and chemotherapy have a role after surgery to treat cancer cells that had already escaped the breast. The same principle applies to MWA. Most patients treated with MWA would benefit from some form of anti-cancer therapy. Women certainly have the right to refuse radiation and medication therapy. However, the primary intent of MWA is to replace surgery, and other measures may be needed to minimize the risk of potential recurrence, especially for larger or more aggressive tumors.